

Search our Blog Posts
Comparing Weight Loss Options
A physician-led guide to medical weight loss, endoscopic procedures, and bariatric surgery options.
Call 978-459-6737 for a consultation, or submit request below

Choosing the right weight-loss treatment
Obesity is a chronic, treatable disease. For many people, long-term weight management requires more than willpower or short-term dieting. Effective treatment may include lifestyle medicine, nutrition support, medication, endoscopic procedures, bariatric surgery, or a combination of these approaches.
At Integrated Gastroenterology Consultants, our Medical Weight Management Center helps patients understand the full range of treatment options. The goal is to match each patient with a safe, evidence-based plan that fits their medical history, weight-related conditions, prior treatment experience, and long-term goals.
IGIC provides physician-supervised weight management for patients in Lowell, Haverhill, Andover, the Merrimack Valley, Southern New Hampshire, and the greater Boston region.
Weight-loss treatment is a continuum
There is no single best weight-loss treatment for everyone. Some patients do well with intensive lifestyle treatment and nutrition counseling. Others benefit from FDA-approved medications. Some need an endoscopic procedure such as endoscopic sleeve gastroplasty or intragastric balloon therapy. Others are best served by bariatric surgery.
A comprehensive program allows patients to consider these options thoughtfully rather than viewing them as competing or unrelated treatments.
Treatment Options Comparison
| Option | How it works | Best suited for | Key considerations |
|---|---|---|---|
| Lifestyle medicine & nutrition support | Structured support for nutrition, physical activity, sleep, stress, and behavior change. | Patients at any stage of weight management. | Foundational for long-term health; may be modest alone but supports all other treatments. |
| Weight-loss medications | Medications may reduce appetite, increase fullness, or affect metabolic signaling. | Patients who meet medical criteria and do not have contraindications. | Non-procedural and adjustable; requires medical supervision. Side effects, access, and coverage vary. |
| Endoscopic sleeve gastroplasty (ESG) | Endoscopic sutures reduce stomach volume without external incisions or stomach removal. | Selected adults seeking a procedural option without traditional bariatric surgery. | Incision-free and minimally invasive; requires anesthesia, staged diet, and follow-up. |
| Intragastric balloon | A temporary balloon is placed in the stomach to promote fullness. | Selected patients seeking a temporary, non-surgical endoscopic option. | Temporary and removable; nausea or intolerance can occur. Long-term success depends on follow-up. |
| TORe after gastric bypass | Endoscopic suturing reduces a dilated gastric bypass outlet in selected patients. | Patients with prior Roux-en-Y gastric bypass and weight regain related to outlet dilation. | Incision-free revision option; only applies to certain post-bypass patients. |
| Bariatric surgery | Surgical procedures alter stomach size and/or digestive anatomy. | Patients with more severe obesity or significant obesity-related conditions. | Often produces the greatest average weight loss; involves surgery, recovery, and lifelong monitoring. |
Lifestyle medicine and nutrition support
Lifestyle treatment is the foundation of obesity care. This does not mean simply advising patients to “eat less and exercise more.” A structured lifestyle medicine approach addresses nutrition, physical activity, sleep, stress, behavior change, medical conditions, and the patient’s day-to-day environment.
At IGIC, lifestyle medicine may include nutrition counseling, health coaching, behavioral strategies, physical activity guidance, and programs designed to support sustainable change. Lifestyle treatment can be used alone or combined with medications, ESG, intragastric balloon therapy, TORe, or bariatric surgery.
Lifestyle treatment may be a good fit for patients who:
Want to focus on metabolic health and long-term behavior change
Prefer to start without medication or procedures
Need support before or after a weight-loss procedure
Have obesity-related conditions such as fatty liver disease, prediabetes, diabetes, high blood pressure, or high cholesterol
Weight-loss medications, including GLP-1 therapies
FDA-approved weight-loss medications can be effective tools for appropriate patients. Some medications, including GLP-1 receptor agonists and related therapies, work by reducing appetite, increasing satiety, slowing stomach emptying, or affecting metabolic signaling.
Medication selection should be individualized. Factors include BMI, medical history, diabetes status, cardiovascular risk, gastrointestinal symptoms, prior medication response, pregnancy considerations, side effects, cost, and insurance coverage.
Weight-loss medications may be a good fit for patients who:
Meet medical criteria for pharmacologic weight management
Prefer a non-procedural option
Have weight-related medical conditions
Need additional support beyond lifestyle treatment alone
May benefit from medication before or after an endoscopic procedure
Important considerations include side effects, medication access, insurance coverage, dose adjustments, and the possibility of weight regain after stopping treatment. Medication therapy should be supervised by a clinician experienced in obesity medicine.
Endoscopic sleeve gastroplasty (ESG)
Endoscopic sleeve gastroplasty is an incision-free procedure performed through an upper endoscope. Sutures are placed inside the stomach to reduce its functional volume and create a narrower, sleeve-like shape. The goal is to help patients feel full with smaller meals and support long-term weight loss when paired with structured follow-up.
ESG may be a good fit for selected adults with obesity who:
Want a procedural treatment but prefer to avoid traditional surgery
Have not achieved durable weight loss with lifestyle treatment alone
Are not ideal candidates for bariatric surgery or do not wish to pursue surgery
Are willing to follow a staged diet and long-term weight management plan
Understand that ESG is a tool, not a stand-alone cure
ESG may be especially relevant for patients who are looking for an option between medication therapy and bariatric surgery. It can also be combined with obesity medications in selected cases.
Intragastric balloon therapy
An intragastric balloon is a temporary, non-surgical device placed in the stomach to promote fullness and help patients reduce food intake. The balloon remains in place for a defined period and is then removed.
Balloon therapy may be a good fit for selected patients who:
Prefer a temporary endoscopic option
Want support initiating weight loss
Are committed to nutrition and lifestyle follow-up
May not be ready for a more durable procedure such as ESG or bariatric surgery
Because the balloon is temporary, long-term success depends on maintaining changes after balloon removal.
TORe for weight regain after gastric bypass
Transoral outlet reduction, or TORe, is an endoscopic procedure for selected patients who have regained weight after Roux-en-Y gastric bypass. In some patients, the connection between the stomach pouch and small intestine, called the gastrojejunal outlet, stretches over time. TORe uses endoscopic suturing to reduce the outlet size and help restore restriction.
TORe may be a good fit for patients who:
Previously had Roux-en-Y gastric bypass
Have experienced weight regain
Have an enlarged outlet or anatomy that may respond to endoscopic revision
Want an incision-free alternative to surgical revision
TORe is not a general weight-loss procedure for patients who have not had gastric bypass. An endoscopic evaluation is needed to determine whether it is appropriate.
Bariatric surgery
Bariatric surgery includes procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass. These operations can produce substantial and durable weight loss and may significantly improve obesity-related conditions such as type 2 diabetes, high blood pressure, sleep apnea, and fatty liver disease.
Bariatric surgery may be the best option for patients with more severe obesity, significant metabolic disease, or a need for the most powerful available weight-loss intervention. Surgery also requires careful preparation, recovery, and lifelong nutritional monitoring.
At IGIC, patients who may benefit from bariatric surgery can be evaluated within a broader medical and endoscopic weight management program and coordinated with surgical partners at Lowell General Hospital and Lawrence General Hospital when appropriate.
How to think about ESG vs medications
ESG and medications are different tools, and some patients may benefit from both.
Medications can be adjusted, stopped, or changed over time. They do not require a procedure, but they may require ongoing use to maintain benefit. Some patients experience side effects, difficulty with access, or inadequate response.
ESG is a one-time endoscopic procedure that changes stomach volume without removing stomach tissue. It requires anesthesia, recovery, a staged diet, and long-term follow-up. Some patients may still need medication after ESG, particularly if weight loss plateaus or if metabolic disease remains active.
The question is not simply “ESG or medication?” The more useful question is: “What combination of treatments gives this patient the safest and most durable path toward improved health?”
How to think about ESG vs bariatric surgery
ESG is less invasive than traditional bariatric surgery and does not involve removing part of the stomach. For some patients, that makes it an attractive option. However, bariatric surgery generally produces greater average weight loss and may be the more appropriate treatment for patients with more severe obesity or advanced metabolic disease.
Patients considering ESG should understand both the advantages and limitations of the procedure. Patients considering bariatric surgery should understand the benefits, risks, recovery, and lifelong nutritional monitoring required after surgery.
A physician-led consultation can help clarify which option is most appropriate.
Which option is right for me?
The best treatment depends on several factors:
Current BMI
Weight history and prior weight-loss attempts
Diabetes, fatty liver disease, sleep apnea, hypertension, high cholesterol, or other weight-related conditions
Prior gastrointestinal surgery
Reflux, swallowing problems, ulcers, or other GI conditions
Medication history and side effects
Insurance coverage and cost considerations
Preference regarding medication, procedures, and surgery
Ability to participate in long-term follow-up
A careful evaluation helps avoid both undertreatment and overtreatment. Some patients need more intensive therapy earlier. Others may do well with a stepwise approach.
Why choose IGIC for weight management and bariatric endoscopy?
Integrated Gastroenterology Consultants offers a comprehensive, physician-led program for obesity and metabolic health. Our team includes clinicians with training in gastroenterology, obesity medicine, lifestyle medicine, nutrition, and advanced endoscopic procedures.
This matters because weight management is not just a cosmetic issue or a short-term goal. Obesity can affect the liver, digestive tract, cardiovascular system, endocrine system, joints, sleep, cancer risk, and overall health. A medically supervised program can help patients choose treatment based on health needs rather than trends or one-size-fits-all recommendations.
IGIC offers care for patients throughout Lowell, Haverhill, Andover, Newburyport, and across the Merrimack Valley, Southern New Hampshire, and the greater Boston region.
Frequently asked questions
Are GLP-1 medications better than ESG?
Not necessarily. GLP-1 medications and ESG work differently. Medications can be very effective for appropriate patients but require ongoing treatment and monitoring. ESG is an endoscopic procedure that reduces stomach volume. Some patients may benefit from one approach, and some may benefit from a combination.
Is ESG safer than bariatric surgery?
ESG is less invasive than bariatric surgery because it is performed through the mouth without external incisions and without removing stomach tissue. However, ESG still has risks and requires anesthesia, post-procedure care, and long-term follow-up. Safety depends on patient selection, procedural expertise, and clinical circumstances.
Is a balloon the same as ESG?
No. An intragastric balloon is temporary and must be removed. ESG uses endoscopic suturing to reduce the stomach’s functional volume. Both are endoscopic options, but they differ in durability, mechanism, and candidacy.
What is TORe?
TORe, or transoral outlet reduction, is an endoscopic revision procedure for selected patients who have regained weight after Roux-en-Y gastric bypass. It is not intended for patients who have not had gastric bypass.
Can I have ESG if I am taking a GLP-1 medication?
Possibly. Medication use before or after ESG is individualized. Some patients may stop, continue, or start medication depending on their response, side effects, medical conditions, and treatment goals.
Is weight-loss treatment covered by insurance?
Coverage varies widely by insurance plan and by treatment type. Medications, nutrition visits, endoscopic procedures, and bariatric surgery may have different coverage requirements. Patients should confirm benefits with their insurer and discuss options with IGIC’s billing team, who can discussion options such as payment plans.
Do I need a referral?
Referral requirements depend on insurance and the type of visit. Patients may contact IGIC directly to request a consultation, and the team can help determine the appropriate next step.
Request a weight management consultation
If you are considering medical weight loss, ESG, intragastric balloon therapy, TORe, or bariatric surgery, Integrated Gastroenterology Consultants can help you understand your options.
Our team provides physician-supervised care in Lowell, Haverhill, Andover, and across the Merrimack Valley, Southern New Hampshire, and the greater Boston region.
Call 978-459-6737 to request a Weight Management Consultation.
Sources:
Jirapinyo P, de Moura DTH, Thompson CC, et al. American Society for Gastrointestinal Endoscopy–European Society of Gastrointestinal Endoscopy guideline on endoscopic bariatric and metabolic therapies for adults with obesity. Gastrointestinal Endoscopy. 2024;99(6):867-885.e64.
Abu Dayyeh BK, Bazerbachi F, Vargas EJ, et al. Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity: a multicentre randomised controlled trial. The Lancet. 2022;400(10350):441-451.
U.S. Food and Drug Administration. De Novo Classification Request for APOLLO ESG System, APOLLO ESG SX System, APOLLO REVISE System, and APOLLO REVISE SX System (DEN210045). FDA; 2022.
U.S. Food and Drug Administration. FDA Approves New Medication for Chronic Weight Management. FDA; 2023.
U.S. Food and Drug Administration. ORBERA™ Intragastric Balloon System: Summary of Safety and Effectiveness Data / Premarket Approval P140008. FDA; 2015.
American Society for Metabolic and Bariatric Surgery. Metabolic and Bariatric Surgery. ASMBS.
Eisenberg D, Shikora SA, Aarts E, et al. 2022 American Society for Metabolic and Bariatric Surgery and International Federation for the Surgery of Obesity and Metabolic Disorders: indications for metabolic and bariatric surgery. Surgery for Obesity and Related Diseases. 2022;18(12):1345-1356.
Mayo Clinic. Intragastric balloon: A re-emerging approach for obesity. Mayo Clinic.
Medically reviewed by Supriya Rao, MD
Last reviewed: 4/30/26
Integrated Gastroenterology Consultants Weight Management & Lifestyle Medicine Center
Endoscopic Sleeve Gastroplasty (ESG)
A minimally invasive, incision-free weight-loss procedure offered as part of a comprehensive, physician-led weight management program.
Endoscopic Sleeve Gastroplasty in Massachusetts
Endoscopic sleeve gastroplasty, often called ESG, is a minimally invasive weight-loss procedure performed through an upper endoscope. During the procedure, a specially trained gastroenterologist places sutures from inside the stomach to reduce its functional volume. This can help patients feel full with smaller meals and support meaningful, sustained weight loss when combined with nutrition counseling, lifestyle treatment, and ongoing medical follow-up.
At Integrated Gastroenterology Consultants, ESG is offered through our Weight Management & Lifestyle Medicine Center as part of a comprehensive obesity-care program. Our approach is individualized and physician-led, with treatment options that may include lifestyle medicine, nutrition support, FDA-approved weight-loss medications when appropriate, endoscopic weight-loss procedures, and coordination with bariatric surgery programs when surgery is the best option.
IGIC provides care for patients in Lowell, Haverhill, Andover, Newburyport, and across the Merrimack Valley, Southern New Hampshire, and the greater Boston region.
What is ESG?
ESG is an incision-free endoscopic procedure designed to reduce the size and shape of the stomach without removing any portion of the stomach. The procedure is performed using an endoscope, a flexible tube passed through the mouth while the patient is under anesthesia. Through the endoscope, the physician places a series of sutures inside the stomach to create a narrower, sleeve-like shape.
By reducing the stomach’s functional capacity, ESG can help patients feel satisfied with smaller portions. ESG is not a stand-alone cure for obesity. It is a tool that works best when paired with structured lifestyle support, nutritional counseling, and long-term medical follow-up.
How ESG differs from sleeve gastrectomy
ESG and surgical sleeve gastrectomy both reduce stomach volume, but they are not the same procedure.
Surgical sleeve gastrectomy is a bariatric operation in which a large portion of the stomach is removed. ESG is performed endoscopically, through the mouth, without external incisions and without surgically removing stomach tissue.
For some patients, ESG may offer an option between medical weight management and bariatric surgery. It may be considered by patients who want a more procedural approach than medication or lifestyle treatment alone, but who are not ready for, do not qualify for, or prefer to avoid traditional bariatric surgery. For other patients, bariatric surgery may still be the more appropriate and effective option. The best choice depends on BMI, medical history, weight-related conditions, prior treatments, preferences, and long-term goals.
Who may be a candidate for ESG?
ESG may be appropriate for selected adults with obesity who have not achieved sustained weight loss with lifestyle changes alone. Many ESG studies have focused on patients with a BMI in the range of approximately 30–40, though candidacy depends on the full clinical picture rather than BMI alone.
Patients may be considered for ESG if they:
Have obesity or significant weight-related health concerns
Have tried lifestyle changes but have not achieved adequate or durable weight loss
Prefer an incision-free procedure rather than traditional bariatric surgery
Are willing to participate in structured follow-up after the procedure
Understand that ESG works best as part of a comprehensive treatment plan
ESG may not be appropriate for patients with certain stomach conditions, prior upper gastrointestinal surgery, active ulcers, bleeding disorders, severe reflux or large hiatal hernia in some cases, or medical conditions that make anesthesia or endoscopy unsafe. A consultation is required to determine whether ESG is appropriate.
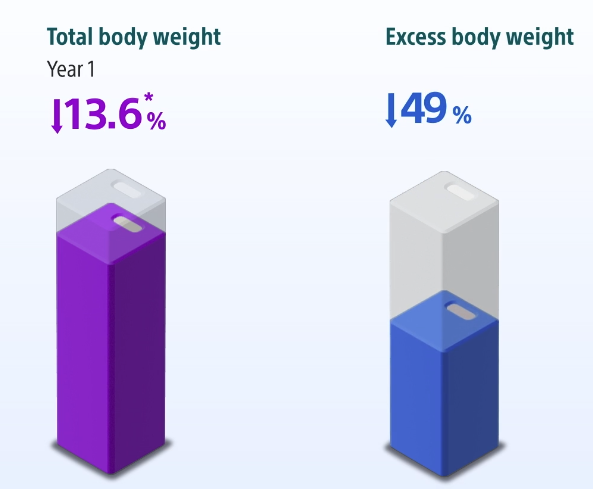
Expected weight loss after ESG
Published clinical studies have shown that ESG can produce meaningful weight loss, particularly when combined with lifestyle intervention and ongoing medical support. Many patients lose approximately 15–20% of total body weight over the first 12–24 months, although individual results vary.
Weight loss after ESG depends on several factors, including starting weight, eating patterns, physical activity, medical conditions, medication use, adherence to follow-up, and the body’s metabolic response to weight loss.
Our goal is not simply short-term weight loss. The purpose of treatment is to support long-term improvement in metabolic health, mobility, quality of life, and obesity-related conditions such as fatty liver disease, type 2 diabetes, hypertension, high cholesterol, and sleep apnea when present.
What happens before ESG?
Before ESG, patients undergo a careful evaluation by the weight management and bariatric endoscopy team. This may include:
A review of weight history and prior weight-loss attempts
Assessment of BMI and obesity-related medical conditions
Medication review
Nutrition and lifestyle assessment
Review of prior gastrointestinal conditions or procedures
Discussion of alternatives, including medications, intragastric balloon, and bariatric surgery
Pre-procedure testing as appropriate
This evaluation helps determine whether ESG is safe, appropriate, and aligned with the patient’s goals.
What happens during the procedure?
ESG is performed with the patient under anesthesia. The physician passes an endoscope through the mouth and into the stomach. Using an endoscopic suturing device, the physician places sutures inside the stomach to reduce its volume and create a narrower configuration.
The procedure is typically performed without external incisions. Many patients go home the same day, although the exact plan depends on the patient’s medical condition and the judgment of the clinical team.
Recovery after ESG
Recovery after ESG is generally shorter than recovery after traditional bariatric surgery, but it still requires careful post-procedure instructions and follow-up. Patients typically follow a staged diet after the procedure, beginning with liquids and gradually advancing as directed by the care team.
Temporary symptoms may include nausea, abdominal discomfort, bloating, cramping, reflux, or difficulty tolerating certain foods early in recovery. The care team provides guidance on hydration, diet progression, medications, activity, and warning signs that should prompt medical attention.
Long-term follow-up is an important part of the treatment. ESG is most effective when paired with structured nutrition support, behavior change, physical activity planning, and medical monitoring.
Risks and safety considerations
ESG is less invasive than traditional bariatric surgery, but it is still a medical procedure and has risks. Potential risks may include bleeding, infection, abdominal pain, nausea, reflux, reaction to anesthesia, leak, perforation, need for hospitalization, or need for additional intervention. Serious complications are uncommon but possible.
The decision to proceed with ESG should be made after a careful discussion of benefits, risks, alternatives, and expectations.
ESG and weight-loss medications
ESG and weight-loss medications are not mutually exclusive. Some patients may benefit from medication before or after ESG, while others may pursue ESG because medication has not been effective, has caused side effects, is not covered by insurance, or is not preferred.
Medications such as GLP-1 receptor agonists and related therapies can be effective for appropriate candidates, but they require medical supervision and may not be suitable for every patient. ESG may be considered as part of a broader treatment strategy that is individualized to the patient’s medical history, treatment response, and long-term goals.
Why choose a gastroenterology-led program?
Obesity is a complex chronic disease, and weight-loss procedures should be performed within a program that understands both gastrointestinal health and long-term metabolic care.
At IGIC, ESG is offered within a coordinated program that includes bariatric endoscopy, obesity medicine, lifestyle medicine, nutrition support, and coordination with surgical partners when appropriate. This allows patients to receive a thoughtful evaluation of the full range of options rather than a one-size-fits-all recommendation.
Dr. Erik Holzwanger, IGIC’s Director of Endoluminal Surgery and Bariatric Endoscopy, as well as Drs. Jaclyn Tuck and Allen Hwang specialize in advanced and minimally invasive endoscopic procedures, including ESG, intragastric balloon, and TORe. IGIC’s Weight Management & Lifestyle Medicine Center also includes clinicians with training in obesity medicine and lifestyle medicine, supporting patients before and after procedures.
Conditions that may improve with weight loss
Weight loss may help improve or reduce the risk of several obesity-related conditions, including:
Type 2 diabetes or insulin resistance
Metabolic dysfunction-associated fatty liver disease
High blood pressure
High cholesterol
Obstructive sleep apnea
Gastroesophageal reflux disease in selected patients
Joint pain related to excess weight
Reduced mobility or exercise tolerance
Cardiovascular risk factors
The effect of ESG on any individual condition varies by patient. Patients should continue routine care with their primary care clinician and relevant specialists.
Frequently asked questions about ESG
Is ESG surgery?
ESG is not surgery. It is an endoscopic procedure performed through the mouth without external incisions and without removing part of the stomach. However, it is still a medical procedure performed under anesthesia and should be considered carefully.
Is ESG the same as sleeve gastrectomy?
No. Sleeve gastrectomy is a surgical bariatric procedure in which part of the stomach is removed. ESG uses endoscopic sutures placed inside the stomach to reduce stomach volume without surgical removal of stomach tissue.
How much weight can I expect to lose after ESG?
Many published studies report approximately 15–20% total body weight loss over 12–24 months, particularly when ESG is combined with structured lifestyle support. Individual results vary.
How long does ESG take?
The procedure is often completed in less than two hours, though timing varies depending on anatomy and clinical circumstances. Many patients return home the same day.
What is the diet after ESG?
Patients follow a staged diet after ESG, usually beginning with liquids and gradually advancing to soft foods and then a long-term nutrition plan. The care team provides specific instructions.
Can ESG be combined with GLP-1 medications?
In some cases, yes. ESG and medication therapy can be complementary. Medication decisions are individualized and depend on medical history, treatment goals, side effects, contraindications, and insurance coverage.
Is ESG covered by insurance?
Coverage varies by insurance plan and may be limited. Our team can help patients understand next steps, but coverage and out-of-pocket costs depend on the specific plan.
Is ESG reversible?
ESG does not remove the stomach, but the sutures and anatomy can change over time. It should not be viewed casually as a temporary procedure. Patients should discuss durability, revision options, and alternatives during consultation.
Who performs ESG at IGIC?
ESG is performed by a gastroenterologist with advanced training in endoluminal surgery and bariatric endoscopy. At IGIC, ESG is performed by Dr. Erik Holzwanger, Director of Endoluminal Surgery and Bariatric Endoscopy; Dr. Jaclyn Tuck, an obesity-certified gastroenterologist with special training in bariatric endoscopy, and Dr. Allen Hwang, an advanced endoscopist with special training in bariatric endoscopy.
How do I know whether ESG, medication, balloon therapy, or surgery is right for me?
The best option depends on BMI, medical history, prior treatments, weight-related conditions, preferences, and long-term goals. A consultation with the weight management team can help determine the most appropriate pathway.
Request a consultation
If you are interested in endoscopic sleeve gastroplasty or other physician-supervised weight-loss options, Integrated Gastroenterology Consultants can help you understand whether ESG is appropriate for you.
Our Weight Management & Lifestyle Medicine Center serves patients in Lowell, Haverhill, Andover, Newburyport, and across the Merrimack Valley, Southern New Hampshire, and the greater Boston region.
Call 978-459-6737 to request a Weight Management Consultation.
Sources:
U.S. Food and Drug Administration. De Novo Classification Request for APOLLO ESG System, APOLLO ESG SX System, APOLLO REVISE System, and APOLLO REVISE SX System (DEN210045). FDA; 2022.
Jirapinyo P, de Moura DTH, Thompson CC, et al. American Society for Gastrointestinal Endoscopy–European Society of Gastrointestinal Endoscopy guideline on endoscopic bariatric and metabolic therapies for adults with obesity. Gastrointestinal Endoscopy. 2024;99(6):867-885.e64.
Abu Dayyeh BK, Bazerbachi F, Vargas EJ, et al. Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity: a multicentre randomised controlled trial. The Lancet. 2022;400(10350):441-451.
Mayo Clinic. Large, multicenter randomized clinical trial examines the safety and efficacy of ESG. Published October 20, 2022.
Medically reviewed by Erik Holzwanger, MD
Last reviewed: 4/30/26
Integrated Gastroenterology Consultants Weight Management & Lifestyle Medicine Center
Peripheral Nerve Evaluation (PNE) for Fecal Incontinence

Do the following sound familiar?
Frequent bowel accidents
Monitoring what and how much you eat
Using pads or protective garments
Planning activities around the bathroom
These are symptoms of fecal incontinence. Unfortunately, many people experience problems with bowel and bladder continence — about 1 in 12 adults in the US has fecal incontinence, and 21 million adults in the US are affected by fecal incontinence. These symptoms can cause problems emotionally, physically, and even socially. Although discussing the problem can be embarrassing, there are a variety of treatment options that the providers at IGIC can offer you. These options can range from simple solutions such as fiber supplementation and optimization of your medications to more nuanced and individualized approaches including physical therapy and neurostimulation.
Our on staff physical therapists have extensive training and expertise in the specific treatment of pelvic floor problems. These are private sessions that focus on your comfort and gradual improvement.
Neurostimulation is an approach to bowel continence problems that focuses on improving the communication that your lower body has with your brain and nervous system.
Our doctors can offer a treatment called Peripheral Nerve Evaluation, or PNE. This is a simple, in-office procedure done with the help of local anesthesia. It requires no preparation and can be done in the order of minutes. During this evaluation, a provider will use a small needle to numb the skin on your back and insert a very thin caliber lead into the tissue under the skin. This lead is then left in place for about one week along with an external stimulator that the patient wears on a belt. During this week, we monitor your symptoms and compare them to the symptoms you had prior to the stimulation.
If the test is successful, which it is in about 70-80% of the appropriately selected patients, we can discuss having a more permanent treatment that can deliver a similar level of stimulation.
Please let your IGIC provider know if you have ever had any problems with bowel continence, such as leakage of stool, frank stool related accidents, or even severe urgency that limits your social interactions and life. Fecal Incontinence (FI) is a treatable condition. It’s not a normal part of aging. And you shouldn’t have to deal with it on your own.
What is Inflammatory Bowel Disease (IBD)?

Types of IBD
There are two main types of IBD:
Ulcerative colitis: This condition causes inflammation in the large intestine (colon), leading to bloody diarrhea.
Crohn's disease: This condition can cause inflammation in the small and/or the large intestine, leading to diarrhea, weight loss, and anemia.
Both ulcerative colitis and Crohn's disease can involve severe diarrhea, abdominal pain, fatigue and weight loss. IBD can be debilitating and sometimes leads to life-threatening complications if untreated.
Symptoms
Signs and symptoms that are common to both Crohn's disease and ulcerative colitis can include:
Diarrhea
Fever and fatigue
Abdominal pain and cramping
Reduced appetite
Unintended weight loss
Diagnosis
Your doctor may perform one or more of the following procedures to diagnose IBD:
Colonoscopy. This exam allows your doctor to view your entire colon using a thin, flexible, lighted tube with an attached camera. During the procedure, your doctor can also take small samples of tissue (biopsy) for laboratory analysis. Sometimes a tissue sample can help confirm a diagnosis.
Flexible sigmoidoscopy. Your doctor uses a slender, flexible, lighted tube to examine the rectum and sigmoid, the last portion of your colon. If your colon is severely inflamed, your doctor may perform this test instead of a full colonoscopy.
Upper endoscopy. In this procedure, your doctor uses a slender, flexible, lighted tube to examine the esophagus, stomach and first part of the small intestine (duodenum). While it is rare for these areas to be involved with Crohn's disease, this test may be recommended if you are having nausea and vomiting, difficulty eating or upper abdominal pain.
Capsule endoscopy. This test is sometimes used to help diagnose Crohn's disease involving your small intestine. You swallow a capsule that has a camera in it. The images are transmitted to a recorder you wear on your belt, after which the capsule exits your body painlessly in your stool. You may still need an endoscopy with a biopsy to confirm a diagnosis of Crohn's disease.
Treatment
The goal of inflammatory bowel disease treatment is to reduce the inflammation that triggers your signs and symptoms. The goal is to achieve not only to symptom relief, but also long-term remission and reduced risk of complications related to untreated IBD. IBD treatment usually involves either life-long medications or surgery. Your doctor will work with you to decide which treatment options are best for you.
Medications
Your doctor will often start you on a short-term steroid medication such as prednisone or budesonide to quickly shut down the inflammation in your intestine. People often start to feel better within days of starting these medications. You will then work with your doctor to decide which long-term medication is best for you. These may include anti-inflammatory drugs such as mesalamine (Asacol HD, Delzicol, Lialda, and others) or a stronger immune suppressant such as azathioprine, mercaptopurine, or methotrexate. In some cases, your doctor may recommend that you start an injection or IV immune suppressing medication. These may include adalimumab (Humira), infliximab (Remicade), vedolizumab (Entyvio), ustekinumab (Stelara), and others. For more information, you can read about these medications through the Crohn’s and Colitis Foundation.
Surgery
For some cases, surgery (removal of the colon or part of the small intestine) may be the best treatment option. This is often when people have not had a good response to multiple medications or for people with Ulcerative Colitis who do not want to be on life-long medication. Your doctor will discuss surgical options with you as well.
If you are concerned you have IBD, call your doctor. You can also call us at 978-459-6737 to request an appointment.